Case 32 : 47 year old male with fever ,headache and altered sensorium
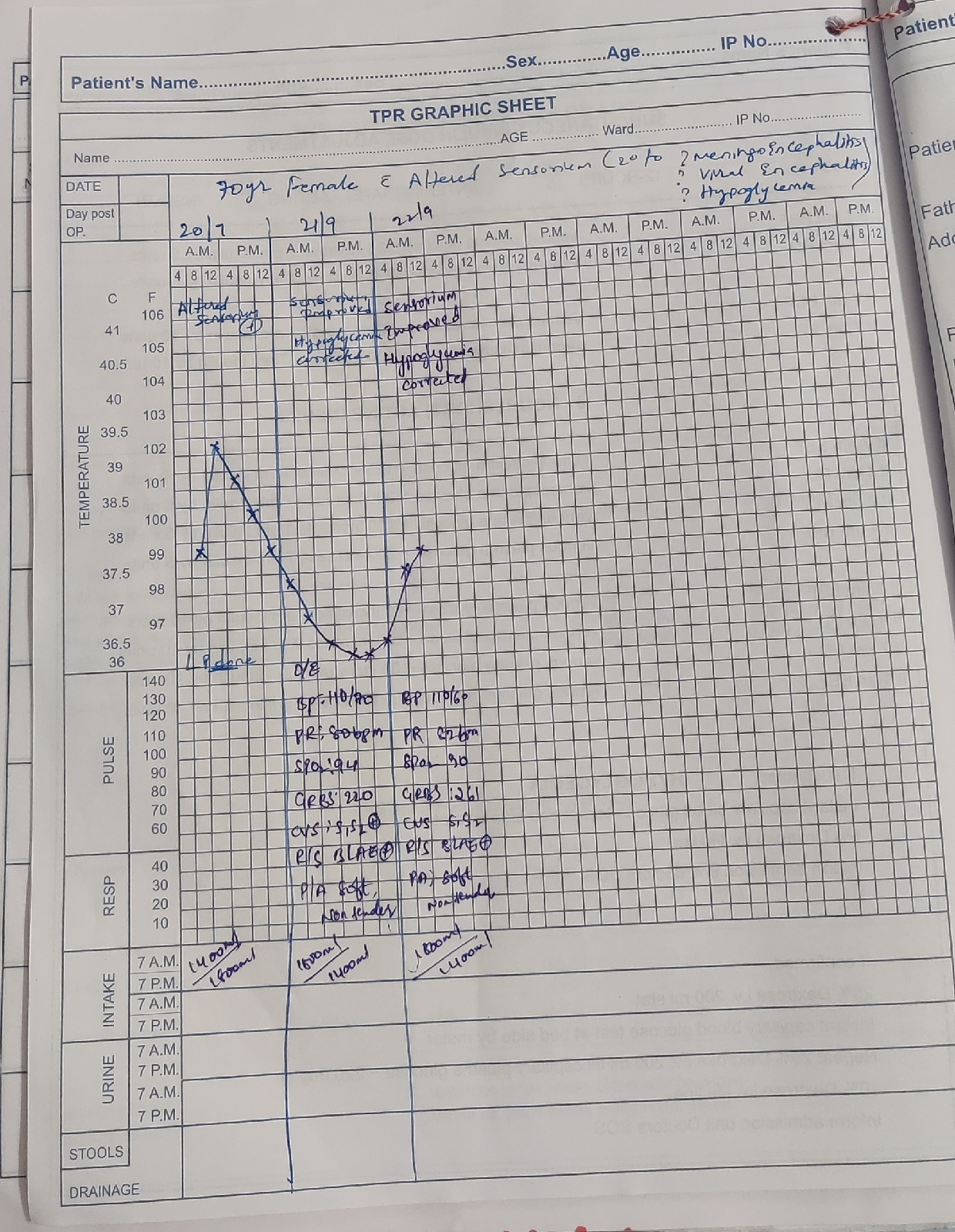
47 year old male with fever ,headache and altered sensorium
thanks DR. Divya raju (intern)
CHIEF COMPLAINTS:
Patient came to the hospital with the chief complaints of - fever , headache , altered talking ,walking n confusion.
HOPI:
Patient was apparently asymptomatic 5days back .Then developed-
High grade fever with chills, intermittent in nature, relieved on medication and was associated with headache.
Altered sensorium since 2 to 3 hours (not talking and not working properly).
No urine output since morning on 24-3-22
No history of burning micturition, vomiting, loose stools, SOB, cough ,chest pain, bleeding manifestations.
pERSONAL HISTORY:
Diet- mixed
Appetite- decreased since 3 days
Sleep - indequate
Bowel - regular
Bladder - decreased urine output on 24-3-22
PAST HISTORY:
N/K/C/O DM ,HTN,BA,TB, CVA,CAD, epilepsy
ADDICTIONS:
Smokes ,montly once and was a occasional drinker but stopped 1 month back.
No significant drug history
FAMILY HISTORY : not significant
GENERAL EXAMINATION:
Patient is oriented to time ,place and person
Poorly built and poorly nourished.
Examined under a well lit room.
No Pallor /Icterus /Cyanosis/clubbing/Edema of feet /Lymphadenopathy.
VITALS :
Temp : 101 F
PR : 90 bpm
BP : 140/80 mmhg
RR : 18
SPO2 : 98 % at RA
GRBS-122 mg/dl
SYSTEMIC EXAMINATION :
CARDIOVASCULAR SYSTEM : S1 and S2 heard, no murmurs heard .
RESPIRATORY SYSTEM : Bilateral air entry present , clear .
PA : soft and non tender
CNS:
GCS-
E4V3M6,
pupils- B/L NSRL
HIGHER MENTAL FUNCTIONS:
- Oriented to time,place,person
- Memory : immediate,recent, remote intact
- Speech: normal
- No delusions or hallucinations
CRANIAL NERVES:
1- normal
2- not tested
3,4,6- No restriction of movement of eye
5-normal( muscles of mastication+sensations of face)
7- normal
8- Normal hearing
9,10- No difficulty in swallowing and speech, gag reflex not tested
11,12- normal.
MOTOR SYSTEM EXAMINATION :
TONE: normal
POWER : Right Left
Upper limb 5/5 5/5
Lower limb 5/5 5/5
Reflexes : Right Left
- Biceps: 2+ 2+
- Triceps: 2+ 2+
- Supinator: 2+ 2+
- Knee: 2+ 2+
- Ankle: 2+ 2+
Plantars: extensor Flexor
Babinski - negative
Meningeal signs-
Neck stiffness -present
Kernigs sign - positive.
SENSORY EXAMINATION:
Normal
CEREBELLUM EXAMINATION:
- Able to do finger nose test.
- Dysdiadokinesia present
- No rebound tenderness
- Gait: could not be elicited
AUTONOMIC NERVOUS SYSTEM:
- No abnormal sweating
- No resting tachycardia



MRI Impression (24-3-22)
- Few lacunar infarcts in medulla on left side.No f/o raised ICT on MRI





Chest x-ray (24-3-22)

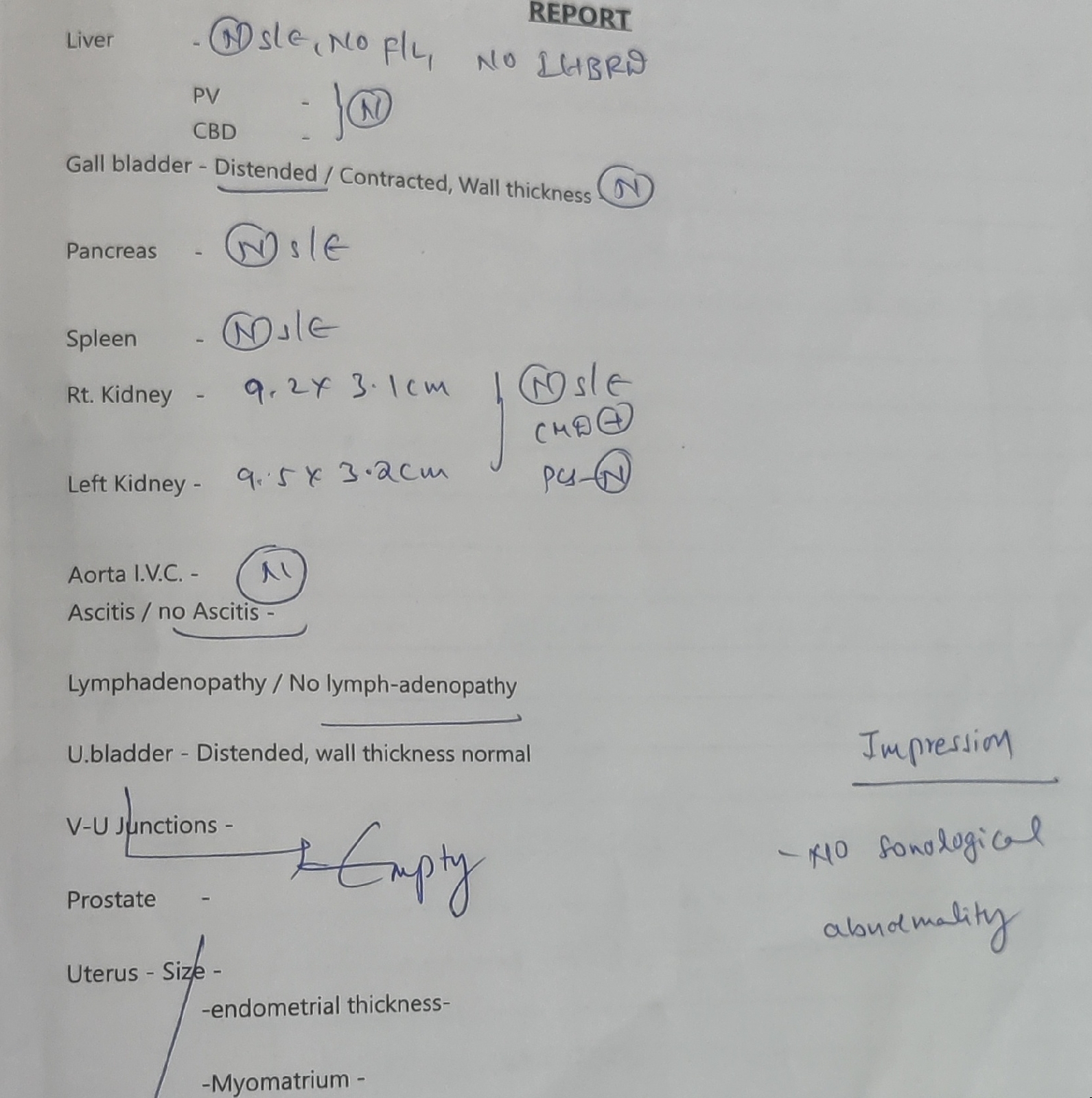
Ultrasound report (24-3-22)
ECG

Opthal- fundoscopy i/v/o any raised ICT for LP



Blood culture report (26-3-22)

Urine culture report(26-3-22)


TREATMENT:
On 24-3-22
IVF NS ,RL ,DNS@100 ml/hr
INJ PANTOP 40 MG IV/OD
INJ.NEOMOL 1 GM IV SOS
INJ. MONOCEF 2 GM IV BD
INJ. DEXA 8 MG IV STAT
TAB DOLO 650 MG RT/SOS
BP,PR monitoring 4 th hourly
On 25-3-22
IVF NS ,RL ,DNS@100 ml/hr
INJ PANTOP 40 MG IV/OD
INJ.NEOMOL 1 GM IV SOS if temp >101°F
INJ.Thiamine 1 amp in 100ml NV/IV/OD
INJ. MONOCEF 2 GM IV BD
INJ. DEXA 4 MG IV STAT
INJ DOXY 100 mg IV BD
Strict I/O charting
W/f seizure activity
INJ. Vancomycin 2mg IV stat
INJ.Optineuron 1amp + 500ml NS over 1hr
BP,PR monitoring 4 th hourly
On 26-3-22
IVF NS ,RL ,DNS@100 ml/hr
INJ PANTOP 40 MG IV/OD
INJ.NEOMOL 1 GM IV SOS
INJ.Thiamine 1 amp in 100ml NV/IV/OD
INJ. MONOCEF 2 GM IV BD
INJ. DEXA 4 MG IV STAT
INJ DOXY 100 mg IV BD
TAB DOLO 650 pO TID
Strict I/O charting
W/f seizure activity
INJ. Vancomycin 1mg IV BD
INJ.Optineuron 1amp + 500ml NS over 1hr
BP,PR monitoring 4 th hourly
On 27-3-22
IVF NS ,RL ,DNS@100 ml/hr
INJ PANTOP 40 MG IV/OD
INJ.NEOMOL 1 GM IV SOS
INJ.Thiamine 200mg IV BD
INJ. MONOCEF 1 GM IV BD
INJ. DEXA 4 MG IV BD
INJ DOXY 100 mg PO BD
TAB DOLO 650 pO TID
Strict I/O charting
W/f seizure activity
INJ. Vancomycin 1mg IV BD
INJ.Optineuron 1amp + 100ml NS over 1hr
BP,PR monitoring 4 th hourly.

LP done on 24-3-22 at 2 am - showing around 450 cells? Lymphocyte predominant,
Glucose - 32
Protein - 195
Chloride - 120
GRBS at time of LP - 112mg/dl
Provisional diagnosis- meningitis?

Comments
Post a Comment