Case 22 - A 55 year old male with altered sensorium under evaluation
This is online E log book to discuss out patients de-identified health data shared after taking his guardian`s informed consent. Here we discuss our individual patient`s problems through series of inputs from available global online community of experts with an aim to solve patients clinical problems with collective current best evidence based inputs. This E log book also reflects my patient centered online learning portfolio and your valuable inputs on comments box is welcome.
A 55 year old male came to op on 4th October with chief complaints of altered sensorium since since one day and history of headache and he took two hypertensive tablets .
History of presenting illness:
The patient was apparently a symptomatic one day back and then he had headache which was sudden in onset and radiating to the neck and he took two tablets of hypertensive medications. Later he developed altered sensorium since evening.patients attenders observed irrelevant behaviour in him since night.
There is no history of chest pain ,palpitations, no involuntary movements, uprolling of eyes,frothing from mouth,deviation of mouth to left side present .
Past history:
CAD Six years back he had chest pain radiating to left arm and was taken to hospital. ECG shown MI pattern ,CABG was done and on medication since then.
Medical history: known case of hypertension since 6 years.
Diabetes : no
Tuberculosis:no
Epilepsy:no
No significant surgically history.
No transfusion of blood.
Personal history:
Diet mixed
Appetite normal bowel and bladder regular
No known allergies
Alcohol occasional
No significant family history.
Non smoker
General examination :patient is conscious but not oriented to place and cooperative.
Pallor no
Icterus no
Cyanosis no
Clubbing no
Lymphadenopathy no
Edema no
Vitals:
Pulse rate 78bpm, regular , normal volume.
Blood pressure 170/90 mm/Hg
Respiratory rate18 cpm
Temperature afebrile
Systemic examination:
CVS:S1 and S2 heart sounds heard.
No murmurs heard
RESPIRATORY SYSTEM
Position of the trachea central
BAE present , vesicular breath sounds heard
Patient is not dyspenic
Abdomen examination

On inspection shape of the abdomen is scaphoid
scar of the previous CABG seen
Palpation: liver and spleen not palpable sand ko palpable masses.
Hernial orifices are free.
No free fluid no bruits
bowel sounds heard.
CNS
Patient is conscious, non coherent , not oriented to place.
Speech : slurred
Power U/L L/L
Right 3/5 3/5
Left 5/5 5/5
Tone U/L L/L
Right Decreased Decreased
Left Normal Normal
Reflexes Biceps triceps supinator knee ankle
Right 2+ 3+ + + +
Left 3+ 3+ 3+ 2+ 2+
Pupil : NSRL
Conjunctival reflex +
Corneal reflex
No meningeal signs.
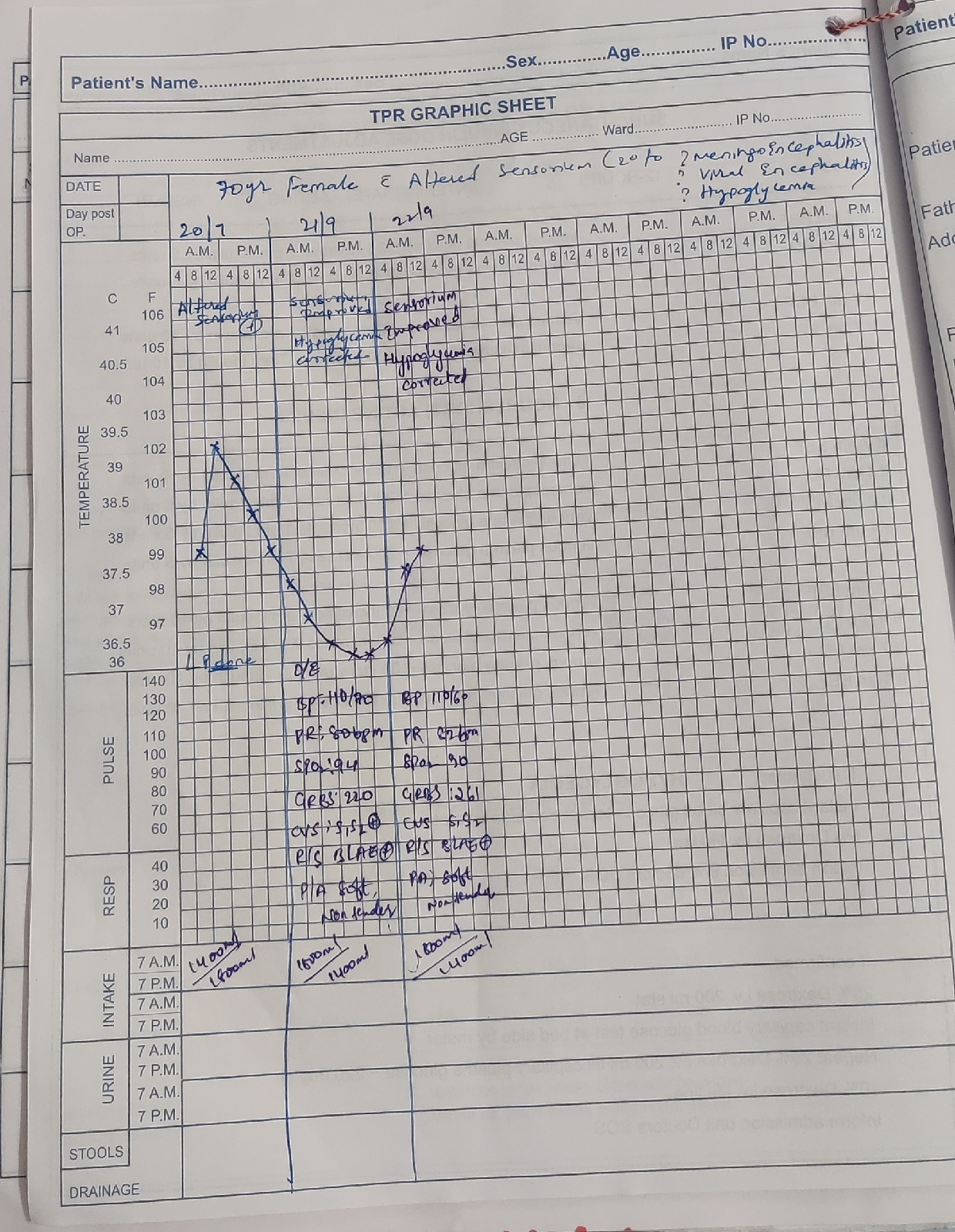
On 8th October
Patient sensorium has improved and responding to commands.
Slurred speech still present
Investigations





Treatment:
1) head end elevation
2)Inj.MANNITOL 100mg IV BD
3)tab.ECOSPIRIN
4)Inj.OPTINEURON I ampoules one NS IV OD
5)tab AMLONG RO /OF at 8:00am
6)physio therapy for right upper limb and right lower limb.


Comments
Post a Comment