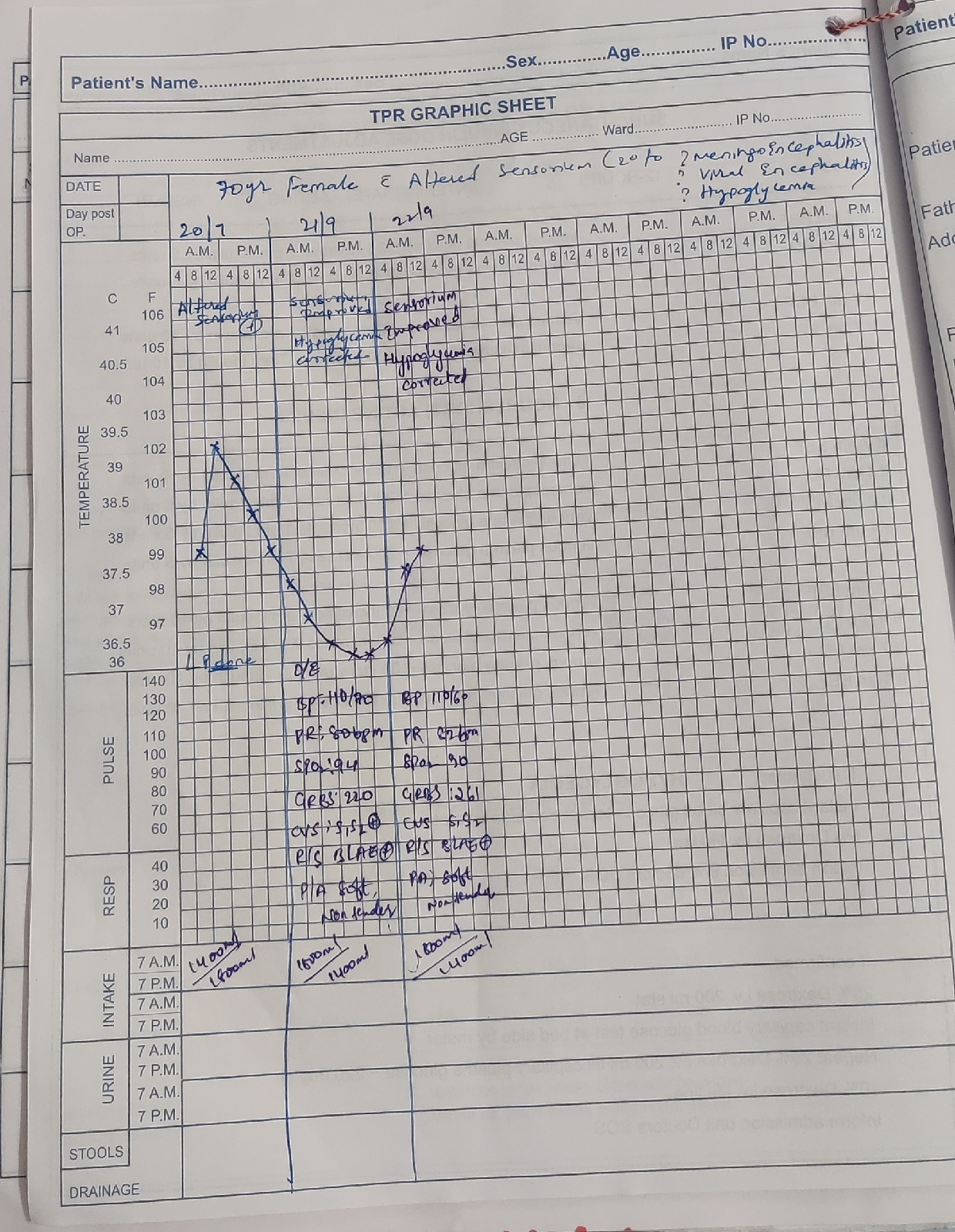
case 2 : 35F with altered sensorium and involuntary movements
Case report
A 35yr old female presented with complaints of vomitings 3 episodes 6 days back followed by altered sensorium .
no h/o trauma
no involuntary movements
no h/o deviation of mouth
no h/o fever,cough,chest pain,tremors,orthopnea,pnd
no h/o use of anticoagulants,oral contraceptive pills
past history:
h/o intermittent headache.
known case of tb 4yrs back ,took ATT for 6 months.
no h/o HTN,DM,CVA,CAD,SIZURES.
surgical history negative.
General examination:
Pallor present
Icterus negative
No cyanosis clubbing lymphademopathy,Edema.
Mild dehydration and malnutrition present .Doll's eye postive
Bp 100/60 mmhg
Pr 110 bpm
spo2 96%
temp 102F
RR 20cpm
Grbs 119 gm/dl
Cvs s1 s2 hears no murmurs
Rs bae + nvbs hears
P/a soft ,nontender,bowels sound heard,
Cns HMF- patient unconscious
stuporous
speech- no response
MMSE- not elicited
cranial nerves-1st not elicited
2nd not elicited
rt lf
3rd,4th,6th
pupil size. N N
DLR/CLR. N. N
NO pstosis, nystagmus.
5th sensory not elicited
motor not elicited
reflex corneal normal,conjuctival normal
7th motor nasolabial fold normal
no deviation of mouth
sensory not elicited
reflex corenal and conjuctival normal
secretomotor moistness of eye and tongue normal,buccal mucosa normal
8 the nerve:Rinnes and Weber's not elicited
9and 10 th nerve: uvula centrally placed,gag reflex present
11 th nerve: trapezieus not elicited, sternocleidomastoid not elicited
12 th nerve: tongue tone normal, no wasting, no fibrillations,no deviation of tongue
MOTOR SYSTEM
Right. Left
Bulk: normal. Normal
Tone: ul. N/ decre. Normal
LL. Decre. Normal
Power not elicited. 3/5 both upper and lower limb
Reflexes.
Superficial reflexes
Right. Left
Corneal. P P
Conjunctival P. P
Abdominal. P. P
Plantar increase. Withdrawal
Deep tendon reflexes
Right. Left
Biceps. P. P
Triceps. N. N
Supinator. N. N
Knee N. N
Ankle. N. N
Primitive reflex -absent
Involuntary movements - absent ( chorea,ballismus - negative) but left lower limb continuous / intermittent movements positive
SENSORY SYSTEM
not elicited
Pain present in all four limbs
CEREBELLUM
titubation - absent
Nystagmus- absent
Intensional tremors - absent
Pendular knee jerk - absent
Coordination test not done
MENINGIAL SIGNS
Neck stiffness - positive
Kernigns sign - negative
Brudzinkis sign - negative
MRI WAS DONE WHICH SHOWED CAPSULOGANGLIONIC HAEMORRHAGE





Course in hospital:The patient was admitted in our ICU with high grade fever spikes and severe leucocytosis suggestive of sepsis along with a mass lesion and hematoma and she was empirically managed with iv antibiotics and her fever spikes and leucocytosis recovered. Her coma took a few more days to recover spontaneously and she was finally able to mobilize herself with persistent neurological deficits since last few days. She still has mutism due to an affection of the Broca's area (insert into the diagnosis) and possible other cognitive deficits yet to be ascertained.
Psychiatry referral was done in view of cognitive function and higher mental functions
According to informent :-
C/o not talking only responding at times
Stressors + (financial, family, personal)
Crying spells + low mood+ ,she was active at work
GAB patient is lying on bed unable to move her right arm and leg
ETEC +, built not sustained
PMA decreased
Rapport could not be established
SPEECH:not uttering words but responding to sounds at times non verbal communication +at times though a bit slow
AFFECT: dysphoric
Further MSE could not be elicited , Orientation could not be assessed
Patient power gradually improved from 0/5 on right side to 3/5 and on left side from 3/5 to 4/5
INVESTIGATIONS
HBS AG: negative
ANTIHCV ANTIBODIES: nonreactive
HIV : non reactive
HEMOGRAM :
28/4 29/4. 1/5. 3/5
HB 5.4 6.3. 7.1. 9.4
Platelets 1.94. 0.31. 1.11. 1.5
TLC 12000
PT. 20. 16
INR. 1.7. 1.1
APTT. 34
BT. 10. 2
CT. 15. 4
TO.BIL. 1.03. 1.48
DI.BIL. 0.27. 0.33
SGOT. 17. 20
SGPT. 8.8. 12
ALK.PH. 68. 64
TO.PRO. 7. 7.1
ALB. 4.1
A/G RATIO. 1.37
RFT
UREA. 17. 52
CREATININE. 0.89. 0.8
URIC ACID 2.6
CALCIUM. 10.5
PHOS. 4.2
SODIUM. 146
K+. 3.6
CL-. 100
2 packs of RDP and 1pack of PRBC transfused on 30/4/20
Diagnosis
Cva with right sided hemiplegia acute haemorrhage involving left corona radiata and lentiform nucleus,internal capsule with intraventricular extension.secondary to ? AV malformations
Acute hemorrhage with ?underlying mass lesion or abscesswith anaemia with old pulmonary Koch's, bed sore resolving ,pseudodementia
?Post stroke delirium
TREATMENT
1) inj. Amikacin 500mg bd
2) inj ceftriaxone 2gm iv bd( both antibiotics were given for 7 days and as sepsis resolved they were de escalated)
2)INJ.Pantop 40 mg od
4) INJ.NEOMOL 1 g IV.( if temp is more than 102F)
5)TAB.PCM 650 mg RT TID
6) INJ.ZOFER 4mg IV.SOS
7)TAB.VITAMIN C 500 mg RT OD
8) TAB. B COMPLEX RT OD
10)TAB.EPTON 100mg RT BD ( Dose slowly tapered as not indicated in seizure prophylaxis in a patient with ICH)
11) SYP.LACTULOSE 10 ml RT TID
12) NEB WITH MUCOMIST 6 TH HOURLY followed by oral suctioning.
13) PROPPED UP POSITION
14) RT FEEDS 2ND HOURLY MILK 30ml
1 HOURLY WATER 150ml
15)I/O CHARTING
16)GRBS CHARTING 6TH HOURLY
17)BP ,PULSE ,SPO2 ,RRMONITORING
18) AIR BED
19)DVT STOCKING
20)FREQUENT CHANGE OF POSITION 2NDHOURLY
21) TEMPERATURE CHARTING 6th hourly.
22)T.FLUOXETINE 20 MG OD× 10 DAYS
23)T.DONAMEM 10MG OD× 10 DAYS
24) Air bed with frequent change of position
25)Bed sores dressing with neosporin powder for l/a
26) CHEST,UPPER AND LOWER LIMBS PHYSIOTHERAPY
PROCEDURE
2D ECHO was done to a heart failure patient with tricuspid regurgitation
And mitral stenosis.
https://drive.google.com/file/d/1XVUkpLrBrsbNkFu-3xeB0Ia2JI9IgeCm/view?usp=drivesdk