case 44 : 35M altered sensorium and seizures
thanks DR. Alekya (intern)
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case presentation:
35yr old male, a lorry driver by occupation came with complaints of involuntary movements of bilateral upper and lower limbs @arount 6AM yesterday.
Pt was apparently asymptomatic before the attack and was watching tv .suddenly patient collapsed and had involuntary movements of bilateral upper and lower limbs tonic- clonic type lasting for 15min. Associated with uprolling of eyes and involuntary passage of urine.
No h/o frothing, tounge bite, deviation of tounge.
Single episode of seizure present according to pts history. Post ictal confusion lasting for about 5hrs.
Pt. Came to casuality in comatose state with respiratory distress. Saturation was maitaining. GCS on arriving is 3/15.
H/o shortness of breath present 3days ago, grade 1 to 2. For which pt. Went to RMP got some medication(not specified by his attenders) and got releived.
Past history :-
* no similar complaints in the past.
no history of head trauma, outside poison intake,
- No h/o headache , fever, vomitings, loose stools, blurring of vision, decreased urine output, pedal edema, chest pains and palpitations.
Not a k/c/o HTN, DM, TB, ASTHMA, CAD, CKD.
He had adequate sleep, regular bowel and bladder habits. Chronic alcoholic 90ml/day ( last binge 3days ago). Non smoker but a tobacco chewer.
No significant family history
Foleys catheterisarion done. Ryles tube was placed.
Vitals:- temp - 103 .5F.,
BP- 100/60,
PR- 108bom, irregularly irregular,varied volume
Atria firing at eg-200 from ectopic foci of dilated myocardium,vagal inhibition on av node-av nodal block-2:1,only 100 beats from ventricles,
These foci can produce variable impulses from atria,av node variable block, ventricles variable beats-> therefore irregularly irregular pulse.
Rr- 39cpm, SpO2 - 96% on 8litres of O2
Grbs-120gm/dl.
GCS --3/15 .. E1V1M1
CNS-
Pupils-dilated and fixed
Tone- R. L
UL-. Normal - hypotonia in both limbs
LL-. Normal- hypotonia in both the limbs.
Reflexes-
Corneal and conjunctival reflexes-present
R. L
Triceps-. +++ +++
Biceps-. - -
Knee. +++. . +++
Ankle-. +++ +++
Plantar- mute
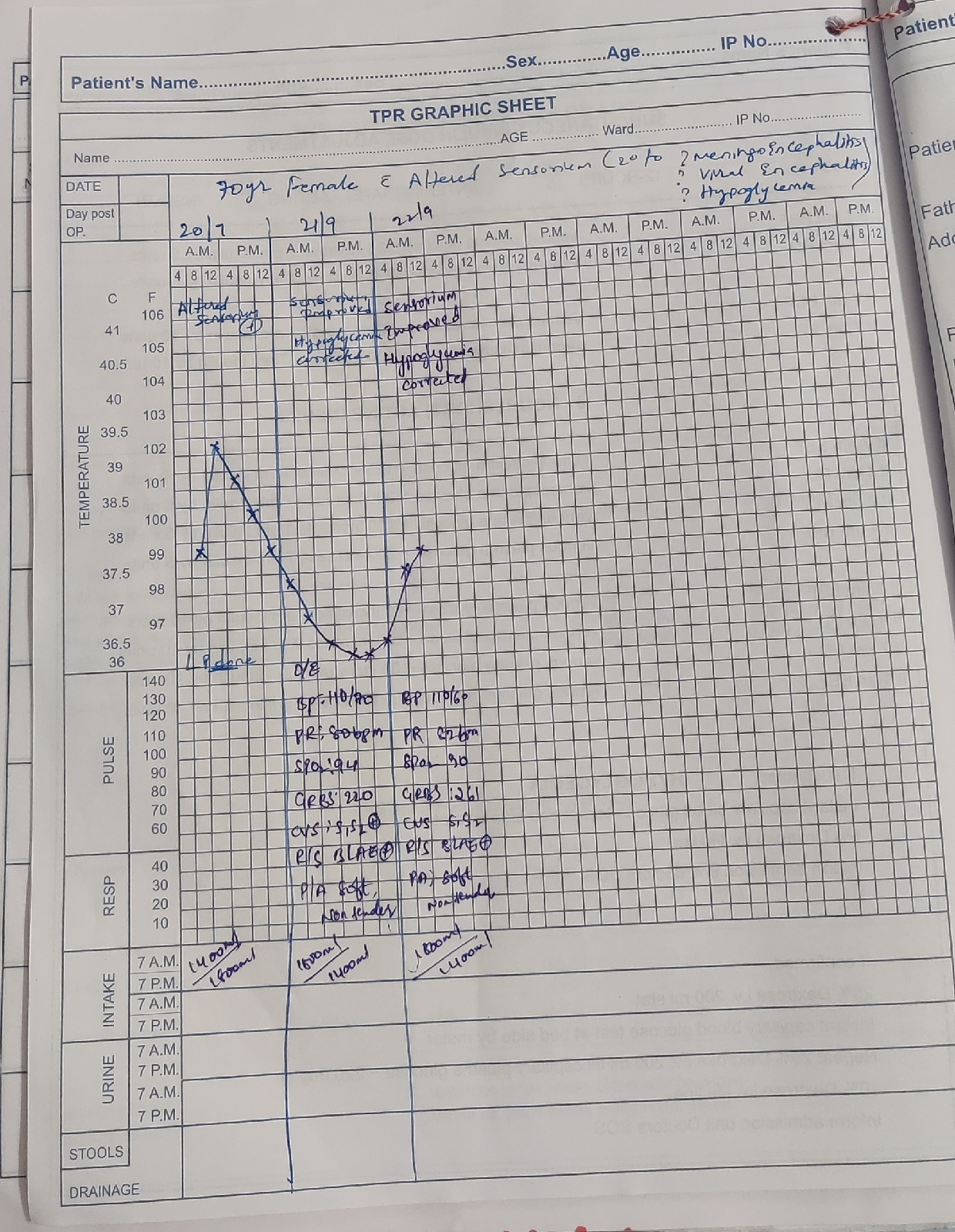
Fever charting-
Day 2

Day4-


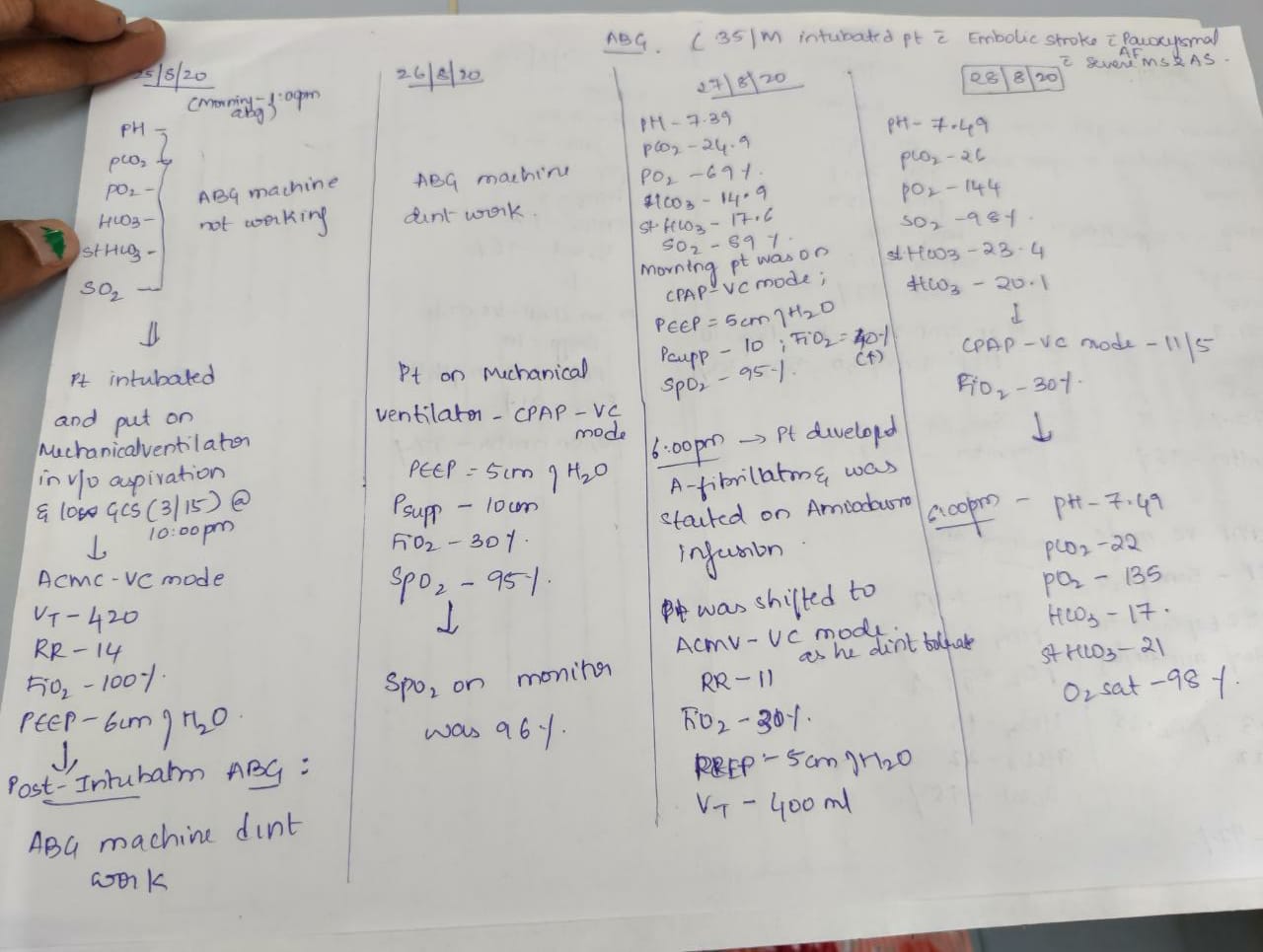

Investigations-
Ecg, CXR-



- Irregularly irregular rhythm.
- No P waves

Ecg on day 7-


Mri brain-













http://pacs.kaminenihospitals.com:99/WADO/MetaData?aet=AEKIMS&studyUID=1.3.12.2.1107.5.2.40.38559.30000020082609335470300000001&sessionKey=a8d61383-37ce-43f0-9b4b-fd535ca49d2f&src=Vijaya

Color- colourless
Appearance-clear
Total count- no cells seen
Hemogram, RFT-


Treatment:-
O2 inhalation
Inj. Levipil 1gm iv stat
Inj. Pan 40mg iv stat.
Inj. Ceftriaxone 2g iv bd
Inj. Zofer 4mg
Inj. Mannitol 100ml iv
Inj. Neomol 100ml
Inj. Thiamine 500mg in 100ml NS iv tid
Inj. Acyclovir 500mg in 100ml NS iv tid
As the patient condition is not improving Intubation was done @9.30pm. And was pit on Nor- adrenaline infusion initially @2ml/hr in view of low blood pressure(90/60).
*Lumbar puncture done @10.30pm and investigations were sent.
* New orders
Head end elevation
Frequent change of position
Dvt stockings
Inj. Ceftriaxone 1g iv bd
Inj. Vancomycin1g iv bd
Inj. Levipil 1g iv bd
Inj. Mannitol 100ml given for 3 days
Inj. Nor adrenaline @2ml/hr
Inj. Thiamine 100mg in 100ml ns
IV fluids NS and RL
Nebulisation with Duolin, Mucomist, Budecort.
Inj. Dexamethasone 8mg iv tid
Inj. Pan 40mg iv
Inj. Zofer 4mg iv tid
Inj. Neomol 1gm
Tab.PCM 650mg
Ryeles tube feeding (water & protien powder+milk)
Inj. Midazolam 1mg sos.
-added t.amiodarone 100 mg RT tid.

Comments
Post a Comment