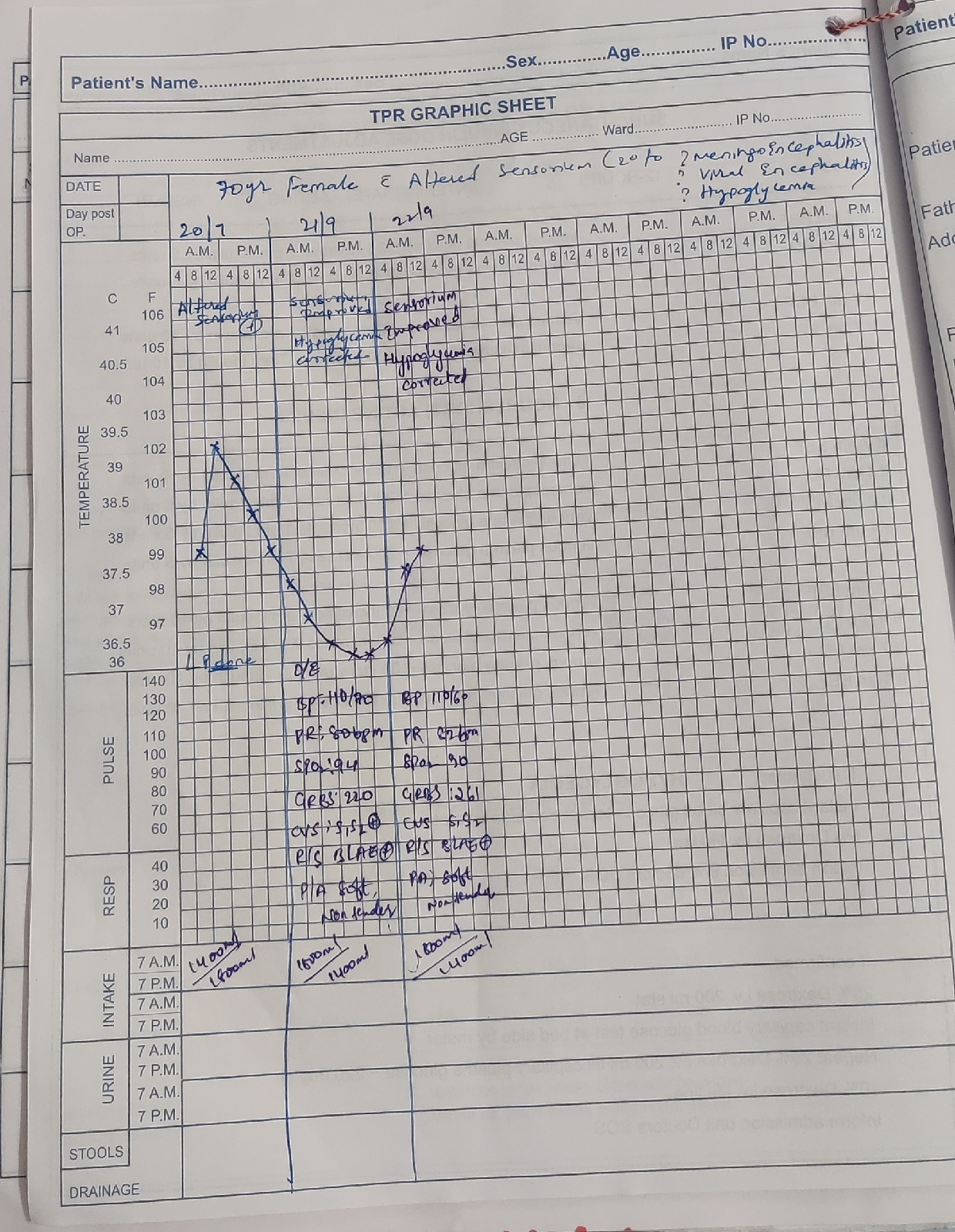
case 12 : 60F with Altered sensorium
thanks sai raghu (intern)
CASE WITH ALTERED SENSORIUM PRESENTED IN SUMMER 2021
- The following E-log aims at discussing our patient de-identified health data shared after taking the guardian's signed consent.
- Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
- This E-log also reflects my patient's centered online learning portfolio.
- I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and providing treatment best to our skills and wisdom.
DRUG HISTORY
➤No significant drug history.
PERSONAL HISTORY
➤Patient takes mixed diet but has a decreased appetite.
➤Bowel and bladder movement is normal and regular.
➤Self care and hygiene not maintained
➤Alcohol consumption 10 years occasionally once in a month (180ml whiskey)
But stopped alcohol intake 6 months back.
➤H/O of consumption of tobacco leaves for the past 5 years (2-3 leaves per day)
FAMILY HISTORY
➤No family history of psychiatric illness.
ALLERGIC HISTORY
➤No significant allergic history
GENERAL EXAMINATION
➤Pallor : Not seen
➤Icterus : Not seen
➤Cyanosis : Not seen
➤Clubbing : Not seen
➤Lymphadenopathy : Not seen
➤Edema : Not seen
➤Malnutrition : Not seen
➤Dehydration: Present
VITALS
➤Temperature : 98.4℉
➤PR : 84 beats per minute
➤BP : 130/70 mmHg
➤RR : 18 cycles per minute
➤SpO2 : 99% in room air
➤Blood Sugar (random) : 186 mg/dl
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM EXAMINATION
➤s1 and s2 heard
➤Thrills absent
➤No cardiac murmurs
RESPIRATORY SYSTEM
➤Normal vesicular breath sounds heard.
➤Bilateral air entry present
ABDOMINAL EXAMINATION
➤Abdomen is soft
➤Non tender
➤No palpable mass
➤Bowel sounds are heard
CENTRAL NERVOUS SYSTEM
Intellectual functions
-patient is conscious,oriented to time ,place and person
-memory-immediate,recent and remote memory present
-appearence-well kept
-speech-normal
2)cranial nerves
Olfactory-smell present on both sides
Optic-visual acuity -6/6
Visual field,colour vision,reflexes -normal
3,4,6 cranial nerves-ocular movements -present
Nystagmus,pros is,Diplopoda-absent
Pupils are normal
Trigeminal -motor and sensory functions normal on both sides
Facial nerve
-No deviation of mouth
-frowning present
-absent nasolabial folds on left side
-blowing and whistling absent
Taste sensation on anterior 2/3rd of tongue present
Corneal reflexpresent on both sides
Vestibulocochlear nerve-rinnes Weber,schwabach test Negative on both sides
Vagus and glossopharyngeal -uvula midline
Spinal accessory-shrugging of shoulders present
Hypoglossal-no deviation of tongue
3)Motor system
A)attitude and position-Normal
B)bulk-no wasting
C)tone-Rt Lt
UL N N
LL N N
D)power-
UL Rt Lt
-5/5 -5/5
LL -5/5 4/5
4)Reflexes
Superficial Rt Lt
Corneal +2 +2
Conjunctival +2 +2
Abdominal +2 +2
Deep Rt Lt
Biceps +2 +3
Triceps +2 +2
Supinator +2 +2
Knee +2 +2
Ankle +2 +2
5)Sensory system
Superficial -fine touch,temperature,pain -present
Deep-position,vibration,crude touch,stereognosis,2point discrimination- present
6)Cerebellum
Speech,nystagmus,ataxia,tremors,released reflexes absent
7)Coordination and gait
Finger nose test ,finger finger test,heel knee test-present
Gait -Normal type
Romberg test -negative
8)signs of meningeal irritation
Nuchal rigidity,kernigs and brudzinski’s sign - absent
PROVISIONAL DIAGNOSIS : ALTERED SENSORIUM SECONDARY TO HYPONATREMIA SECONDARY TO VOMITING
INVESTIGATIONS :
DAY 1
 |
| NORMAL |
 |
| MILDLY ELEVATED |
 |
| HYPONATREMIA-130mEq/L |
 |
| NORMAL |
 |
| NORMAL |
 |
| DECREASED LEVEL OF PROTEIN - 5.1g/dl |
 |
| SERUM BILIRUBIN IS MILDLY ELEVATED |
 |
| SGPT IS NORMAL |
 |
| S.CREATININE IS NORMAL |
 |
| HB is decreased10.6g/dl TOTAL COUNT IS ELEVATED-12,900cells/cumm |
DAY 3
 |
| CHEST X-RAY AP VIEW |
DAY 1
➤Patient was referred to psychiatry department for cross consultation.



➤Patient was not cooperative
➤Na- 130 mEq/L
➤Potassium - 3.6 mEq/L
➤Chloride-97mEq/L
➤Hb-10.6g/dl
➤WBC- 12900 cells/cumm
1) TAB.CLONAZEPAM 0.5mg BD
DAY 2
➤C/O headache
➤Fever spikes absent
➤PR-98 beats/min
➤BP-130/80mm of Hg
➤GRBS-135mg/dl
TREATMENT
1) INJ.3% NaCl continuous infusion @ 15 ml/hour
2) INJ. PAN 40mg IV/OD
3) INJ.ZOFER 4mg IV/TD
4) ORS sachets 2 in 1 litre
5) BP/PR/TEMP./SpO2 montoring
DAY 3
➤C/O headache
➤Fever spikes absent
➤Patient is conscious and irritable
➤PR-78 bpm
➤BP-160/100 mm of Hg
➤Patient was referred to ophthalmology department for cross consultation
 |
| No view of fundus in both eyes due to dense cataract |
TREATMENT
1) INJ.3% NaCl continuous infusion @ 15 ml/hour
2) INJ. PAN 40mg IV/OD
3) INJ.ZOFER 4mg IV/TD
4) ORS sachets 2 in 1 litre
5) BP/PR/TEMP./SpO2 montoring
DAY 4
➤Headache decreases
➤Fever spikes absent
➤Stools passed
➤Patient is conscious ,coherent and cooperative.
➤PR-86 bpm
➤BP-130/80 mm of Hg
➤GRBS-211 mg/dl
TREATMENT
1) INJ.3% NaCl continuous infusion @ 15 ml/hour
2) INJ. PAN 40mg IV/OD
3) IV fluids NS @ 100 ml/hour
4) TAB.PCM 650mg TID
5) INJ.ZOFER 4mg IV/TD
6) ORS sachets 2 in 1 litre
7) BP/PR/TEMP./SpO2 montoring

Comments
Post a Comment