case 11 : 26M Altered Sensoriumand seizures
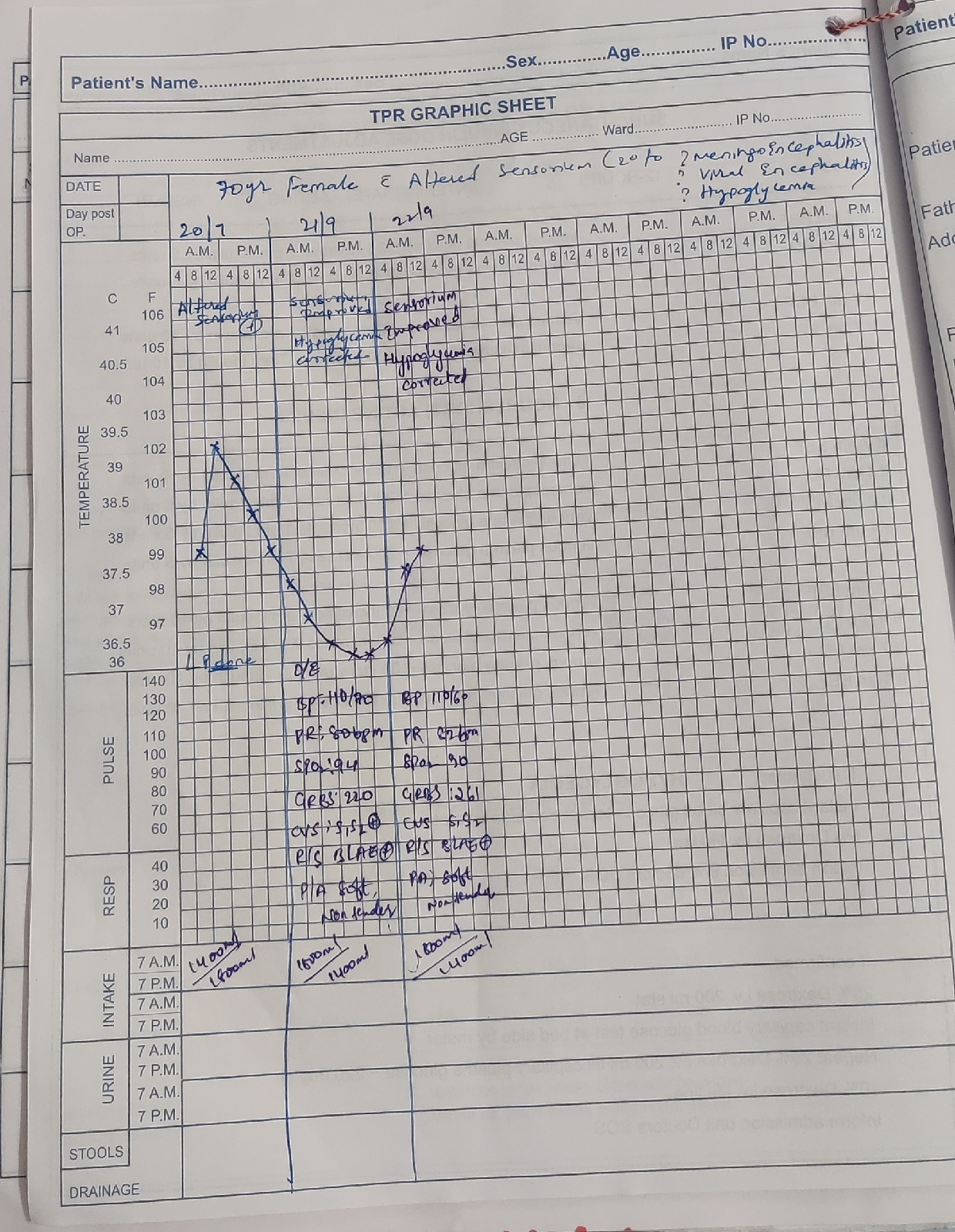
A CASE OF B/L PEDAL EDEMA, ALTERED SENSORIUM AND DYSPNEA.
92 Sneha Nadipi
3rd Semester
Under the guidance of Dr.Pavan Kalyan(intern).
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
🖌This is an ongoing case. This blog post will be updated regularly.
- Married
- Occupation : Driver
- Apettite loss:No
- Bowels : irregular
- Micturition : Decresed
- No H/O known drug allergies
-Alcohol : regular (7 years)
-Tobacco -Yes
🌡PHYSICAL EXAMINATION :
A) GENERAL EXAMINATION :
- Pallor- NO
- lcterus-YES
- Cyanosis-No.
- Clubbing of fingers/toes- No
- Lymphadenopathy-No
-Oedema of feet- YES(B/L PEDAL EDEMA)
-Pupils-B/L pupils dilated
- Malnutrition - No
-Dehydration -NO
- No H/O pallor, cyanosis , lymphadenopathy , clubbing of fingers or toes , dehydration
- Temperature : Afebrile
- BP : 70\50 mmHg
- PR : 49 BPM
- SPO2 : 85% at room air
-GRBS:135 m/dl
-RR-36 cpm
🌡SYSTEMIC EXAMINATION:
B) CVS
- Thrills : No
- Cardiac sounds - S1 , S2 heard
- Cardiac murmurs : No
C) RS
- Dyspnea : YES
- Wheeze : No
-Inspiratory crepts-B/L IAA
D) ABDOMEN
- Bowel sounds : YES
E) CNS
- altered sensorium
★ REFLEXES
-Absent
INVESTIGATIONS:
ECG:

X-RAY:

🌡SEROLOGICAL INVESTIGATIONS: ON 25/07/21(OUTSIDE)
Hb-13.8
TLC-14,100
PLT(plateletcount)-51,000
Serum creatinine: 3.7 mg/ dl
Blood urea: 128 mg/ dl
Sodium : 133 mEq/L
potassium : 3.6 mEq/L
chloride : 53 mEq/L
Liver Function Test:
TB -19
DB -7.8
IB-11.2
AST -147
ALT -185
Alkaline Phosphate-135
TP:6.9
Alb-3.7
A/G-1.1
Electrolytes:
Na-155 mmol/lit
K-5.4 mmol/lit
Cl-95 mmol/lit
Blood Glucose Test-PositiveS.lyase -102PT-29 secINR-2.8
APTT-50 sec
Dengue-NEGATIVE
HIV-NEGATIVE
HCV-NEGATIVE
HBS Ag-NEGATIVE
ON 25/7/21(In Hospital)
Hb-13.9
TLC-16,950
PLT(plateletcount)-63,000
Serum creatinine: 2.7 mg/ dl
Blood urea: 89mg/ dl
Sodium : 133 mEq/L
potassium : 3.6 mEq/L
chloride : 53 mEq/L
Liver Function Test:
TB -12.1
DB -2.2
IB-11.2
Utica acid:6.2
AST -680
ALT -140
Alkaline Phosphate-135
TP:5.2
Electrolytes:
Na-120 mmol/lit
K-5.1 mmol/lit
Cl-80 mmol/lit
ABG
pH:7.06
pCO2:18.4 mmHg
pO2-not mentioned
HCO3-7.9 mEq/mol

S.lyase -43
S.Amylase-82
BT:2 min 30 seconds
CT:5 mins
INR-2.0
APTT-57 sec




Hemogram:



- IVF-30 NS
- Inj.THIAMINE 1 amp in 100 ml IV/ID
- Inj. VIT K IV/in 100 ml NS -DD
- Plan for FFP transfusions
- TAB.Udiliv 300 mg po/TID
- Syp . Lactulose 15 ml /po/TID
- Syp. Hepamerz 10 ml/po/BD
- Inj. PIPTAZ 4.5 gm/IV—2.25 gm/IV/TID
- Inj.methyl prednisole 40mg/IV/OD in 100ml NS
- Propped up posture/head end elevation
- TAB.RIFAGUT 500 mg BD/RT
- Inj. PAN 40mg IV/OD
- Oxygen supplementation maintains sPO2>95%
- Monitor vitals-BP hourly
- Strict I/O charting
- Inj. Noradrenaline 12ml/hour infusion
- GRRS charting 6th hourly
- Inj.Vasopressin infusion 2.4 ml/hour
- Inj.LASIX 20mg IV/BD 8 AM - 4PM IF SBP >110 mmHg
- ABG every 6th hourly.

Comments
Post a Comment