case 7 : 45M altered sensorium
45 Y/O MALE WITH COVID-19 AND COMORBIDITIES (ALTERED SENSORIUM, AZOTEMIA, HYPOKALEMIA.)
thanks M.Anurag, MBBS 8th semester

This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and a treatment plan.
(Contains information collated from Dr.Manasa PG and from the patient)
CASE DISCUSSION:
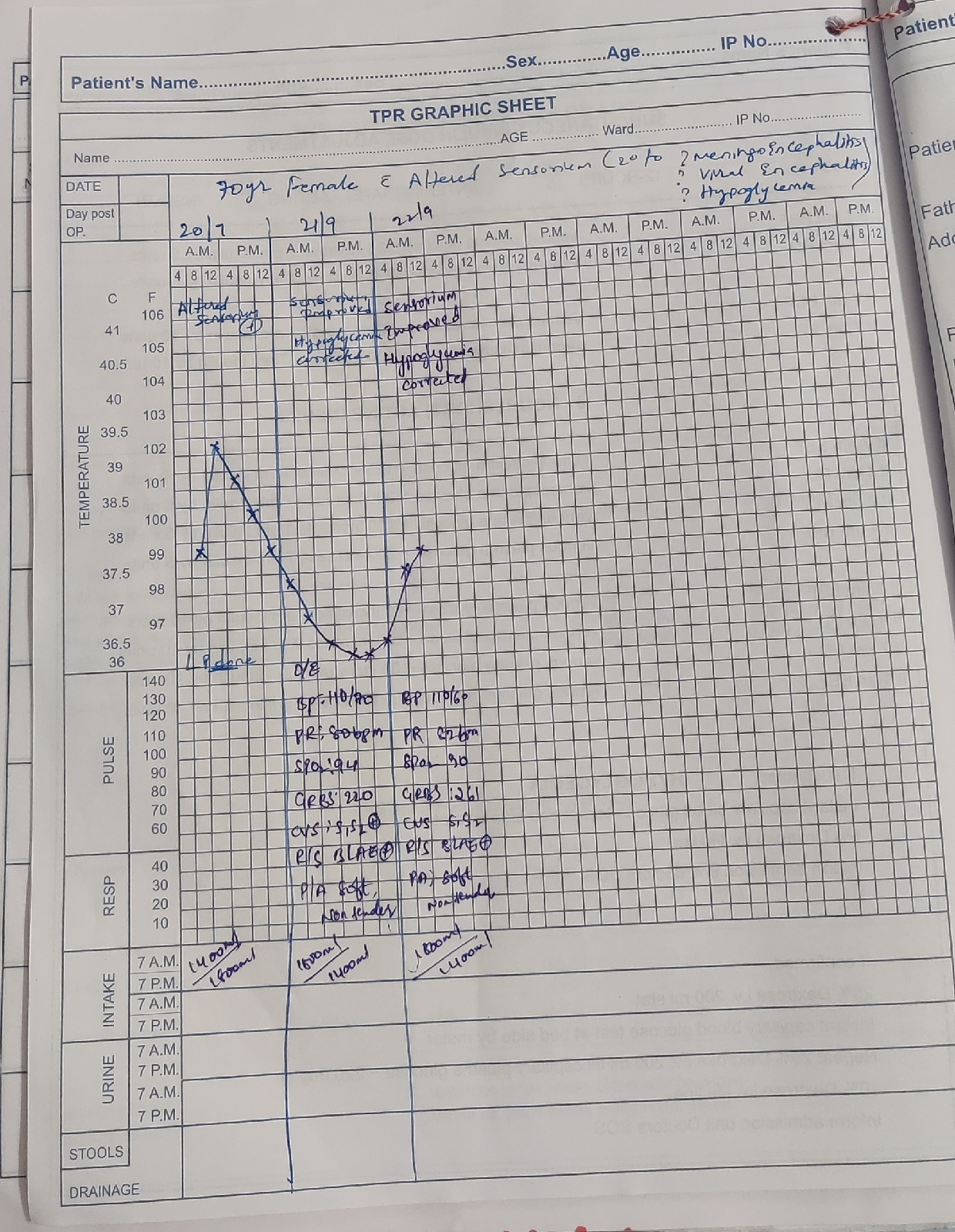
A 45yr old male patient, resident of xxxx , labourer by occupation was brought to the ER on 19-4-21 in an unconscious state with SpO2 20% and the Glasgow Coma Scale score of 3(E1V1M1).
HISTORY OF PRESENTING ILLNESS:
The patient was apparently asymptomatic 2 days ago.Then (on 17-4-21) he developed mild grade fever which was insidious in onset , continuous in character.
It did not have any aggrevating or reliving factors
It was not associated with rash , chills , rigor , vomiting , abdominal pain , or burning micturition.
18-4-21:
The patient developed generalised weakness and myalgia
19-4-21:
The patient developed slurred speech and extreme weakness of all the 4 limbs. Later he became unconscious and was brought to the ER with SpO2 of 20% and a GSC score of 3(E1V1M1)
HISTORY OF PAST ILLNESS:
There were no similar complains in the past.
The patient is not a known case of DM, HTN, CAD, TB or Epilepsy.
No previous surgical history
PERSONAL HISTORY:
DIET:Mixed
APPETITE:Normal
SLEEP:Adequate
BOWEL AND BLADDER MOVEMENTS:Regular
ADDICTIONS:
•The patient is a chronic alcoholic consuming 1 quarter of whisky per night but he stopped consuming alcohol since 2yrs but he again started consuming alcohol occasionally since 3-4 months.
•The patient consumes tobacco in the form of cigarettes smoking 3 chuttas per day since 20 years
NO KNOWN ALLERGIES
FAMILY HISTORY:
No significant family history
DRUG HISTORY:
The patient does not take any drug therapy.
GENERAL EXAMINATION:
The patient was unconscious and had a GCS score of 3
He was moderately built and nourished.
Vitals:
PULSE RATE: 100bpm
BP: 160/100 mm Hg
TEMP: 99.1 degree F
SpO2 AT RA: 30%
GRBS: 322 mg/dl
DEHYDRATION: Mild dehydration present
Pallor: absent
Icterus : absent
Clubbing: absent
Cyanosis: absent
Lymphadenopathy: absent
Edema: absent
SYSTEMIC EXAMINATION:
CVS: S1,S2 heard. No thrills or murmurs
RS: Dyspnoea+, No wheeze
ABDOMEN: Scaphoid shaped and Non tender
Bowel sounds are heard.
CNS:
LEVEL OF CONSCIOUSNESS: Coma
SPEECH: No response
SIGNS OF MENINGEAL IRRITATION: No neck stiffness , Kernig sign -ve
PUPILS: Sluggishly reacting to light
MOTOR SYSTEM:
Tone: Decreased in upper and lower limbs
Power: 0/5 in upper limbs and 2/5 in lower limbs.
INVESTIGATIONS:
COMPLETE BLOOD PICTURE:

Interpretation:
Elevated TLC, Neutrophils, Lymophocytes, MCHC
RENAL FUNCTION TESTS:

Interpretation:
Elevated Urea, Creatinine, Uric acid level. Decreased Potassium levels (Hypokalemia)
LIVER FUNCTION TESTS:

Interpretation:
Elevated Alkaline phosphatase
X-RAY CHEST: 
ECG REPORT:


RAPID ANTIGEN TEST FOR COVID-19 DONE: Patient was tested POSITIVE.
PROVISIONAL DIAGNOSIS:
Information based on above investigations and case history is indicative of viral pneumonia secondary to COVID-19 and comorbidities (altered sensorium, azotemia, hypokalemia)
TREATMENT:
Patient was intubed within 1 hr of admittion in view of the falling SpO2 saturation at 20%
PRE-INTUBATION VITALS:
BP: 160/100 mm Hg
PR: 80bpm,Regular
Pupils: Sluggishly reactive
ABG Report: pH:6.88, pCO2:123, pO2:23.8, S.O2:23.5, HCO3:10.1
POST-INTUBATION VITALS:
BP: 100/60 mm Hg
PR: 100bpm, Regular
ABG Report: pH:7.046, pCO2:67.5, pO2:357, FiO2:100%, S.O2:98.6, HCO3:13.5
DRUG THERAPY IN HOSPITAL:
1)Pre anaesthesic medication: Inj. MIDAZOLAM 2cc iv STAT
2)Inj. ATRACURIUM 2cc iv STAT
3)Inj. GLYCOPYROLLATE 2cc STAT
4)ET tube 7.5mm insertion confirmed with 5 point auscultation
Then the patient was put in a ventilator ambulance and sent to a higher COVID centre.
He was put on mechanical ventilation in the centre, for 3 days and was also diagnosed and treated for Hypokalemic periodic paralysis following which he was discharged after 5 days.
The patient is currently doing fine
HYPOKALEMIC PERIODIC PARALYSIS:
Hypokalemic periodic paralysis (hypoPP or hypoKPP) is a rare disorder in which a person experiences episodes of painless muscle weakness and often paralysis. It’s the most common of several genetic disorders that cause periodic paralysis.
Symptoms:
•heart palpitations
•weak or cramping muscles, most often in the arms, legs, shoulders, and hips
•paralysis
Triggers for the attack:
•sugary or starchy foods
•salty foods
•going too long between meals
•eating a very large meal
•sleep
•high levels of physical exertion
•temperature extremes
•strong emotion
•certain medications, such as anesthesia
Management:
•Carbonic anhydrase inhibitors: These medications increase the flow of potassium. Common options include dichlorphenamide (Keveyis) and acetazolamide (Diamox).
•Potassium supplements: Oral potassium supplements may be given to help stop an attack that’s in progress. Your doctor will advise you on proper dosage.
References:
Research Papers:
1) Review of the Diagnosis and Treatment of Periodic Paralysis
2) Study of incidence and prevalence of Hypokalemic Periodic Paralysis

Comments
Post a Comment