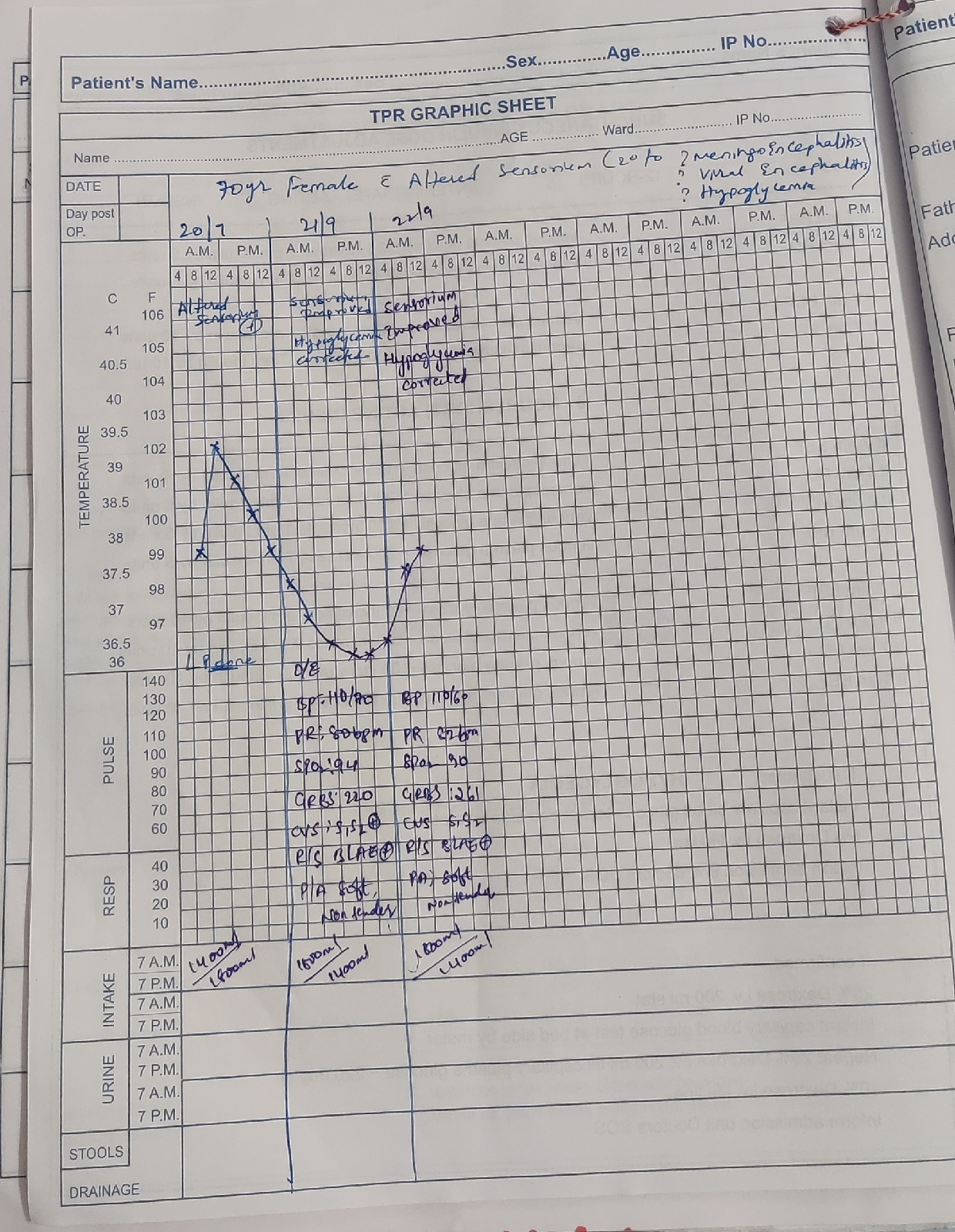
Case 20 - Altered sensorium - SIADH
A 45years man was brought to the casualty in an unresponsive state with fever and chills since 2 days
On presentation, tonic posturing with frothing from mouth, fever and shivering
for seizures- inj lorazepam and levipill were given HOPI- there was a decrease on appetite since 2days, pt was taken to the nearby RMP when he was given iv fluids, with no improvement in symptoms he was reffered here.
Similar complaints 15 days back with UTI, SEPSIS and resolved Alcohol withdrawal seizures
Patient stopped working since 1 year (due to generalized weakness)
2 months back - pt had back pain (occasionally took pain killers).
H/O alcohol consumption since 15yrs(weekly thrice)
Zarda pan consumption - since 15 years Daily 1pack.
No H/O smoking
Not a k/c/o DM, HTN, Asthma,TB, CAD
No H/o any past surgeries
On examination :
Pt is unresponsive E1V1M4
No signs of pallor, icterus, cyanosis, clubbing, lymphadenoapathy, edema
Vitals:
temp- 101 F
PR: 90 bpm, regular
RR: 26 cpm
BP: 90/50 mmHg
SPO2:
AT ROOM AIR 100%
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
CNS examination
Higher mental functions -
GCS - E1V1M4
Cranial nerves -
Pupils - sliggish reacting to light ,mid dilated .
Dolls eye - present
Gag reflex - intact
Motor -
Attitude of limbs -
hypertonia in all four limbs
Power couldn't be elicited as he is comatosed
Spontaneous limb movements observed .
Reflexes -. R L
B. 2+. 2+
T 2+. 2+
S 2+. 2+
K 2+. 2+
A 2+. 2+
Plantars - bilateral extensor
Sensory and cerebellar couldn't be ellicited
As patient is having fever spikes + ,meningeal signs+
LP was tried but couldn't get fluid .
EUVOLEMIC HYPOSMOLAR HYPONATREMIA ?SIADH.
? BACTERIAL/TB MENINGITIS
On lab evaluation he was found to be - severe hyponatremic -
With sodium -117 (Deficit)
serum osmolarity- 241
urine electrolytes-
Cl- 182
Potassium- 16.4
Sodium- 142











management-
FLUID RESTRICTION <1 lit/day.
1 IN. LORAZEPAM acc/iv/stat
2 Inj. LEVIPILL 1000mg iv stat, 500mg iv Bd
3 inj 3% NaCl iv 15ml/hr ( based on s/electrolytes)
4. Inj - OPTINEURON 1amp in 100ml N//IV/00
6. RT FEEDS 200ml milk with protein powder
6. IN. NORADRENALINE 2amp in 45ml NS / 4ml/hr( based on MAP 65mm hg
7. vitals monitoring - PR BP, GRBS, SPO2 4th hourly
ICU bed 4
45yrs/male
SOAP NOTES DAY 1
Subjective
H/o fever spikes
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP 98.2F
PR: 92 bpm, regular
RR: 21cpm
BP: 100/70 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:188mg/dl
Systemic examination :
CVS:S1,S2 heard Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowelsounds hear
Cns:
HMF+
SPEECH-NORMAL
MEMORY-intact Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs) Reflexes
BTSAKP
R 2+ + + + flexion
L 2++++flexion
Assessment
Altered sensorium secondary to ? Hyponatremia- ? SIADH
TB/ Bacterial meningitis With
pyrexia
Plan of care
head end elevation
inj levipil 800mg in bd inj 3% NaCl @ 25ml/hr
inj noradrenaline 2amp in 45ml NS
inj optineuron 1amp
inj monocef 2 lgm iv
inj Vancomycin
Inj tolvaptan
ICU bed 4
45yrs/male
SOAP NOTES DAY 2
Subjective
H/o fever spikes
Objective
On examination :
Pt is c/c/c
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP 98.2F
PR: 82 bpm, regular
RR: 21cpm
BP: 100/70 mmHg
SPO2:
AT ROOM AIR-98%
GRBS:145mg/dl
Systemic examination :
CVS:S1,S2 heard Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowelsounds hear
Cns:
HMF+
SPEECH-NORMAL
MEMORY-intact Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs) Reflexes
BTSAKP
R 2+ + + + flexion
L 2++++flexion
Assessment
Altered sensorium secondary to ? Hyponatremia- ? SIADH
TB/ Bacterial meningitis With
pyrexia
Plan of care
head end elevation
inj levipil 800mg in bd
inj 3% NaCl @ 25ml/hr
inj noradrenaline 2amp in 45ml NS
inj optineuron 1amp
inj monocef 2 lgm iv
inj Vancomycin
Inj tolvaptan

ICU bed 4
45yrs/male
SOAP NOTES DAY 3
Subjective
No fever spikes
Objective
On examination :
Pt is c/c/c
Oriented to t/p/p
patient is able to talk and started oral feed
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals:
TEMP 98.2F
PR: 90 bpm, regular
RR: 15cpm
BP: 110/80 mmHg
SPO2:
AT ROOM AIR-99%
GRBS:101mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-(Normal in all 4 limbs)
Reflexes-
B T S A K P
R 2+ + - + + flexion
L 2+ + - + + flexion
Assessment-
Altered sensorium secondary to ? Hyponatremia- ? SIADH
TB/ Bacterial meningitis With
pyrexia
Plan of care-
head end elevation
inj levipil 800mg in bd
inj optineuron 1amp
inj monocef 2 lgm iv
inj Vancomycin 500mg in 200ml NS
Inj Neomol 1gm iv sos
tab pcm 650mg
tab tolvapt 15mg
double strength Ors
monitoring vitals 4th bourly
.Monitor vitals-4rth hourly
I/O charting


AMC bed 7
45yrs/male
SOAP NOTES DAY 5
Subjective
No fever spikes
Objective
On examination :
Pt is c/c
Oriented to t/p/p
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitals
PR: 86 bpm, regular
RR: 15cpm
BP: 90/70 mmHg
GRBS: 120 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-
Reflexes-
B T S K A P
R 2+ 2 +1+3 -withdrawal
L 2 +2 +1 +2 - withdrawal
Assessment-
Altered sensorium secondary to ? Hyponatremia- ? SIADH
TB/ Bacterial meningitis With
pyrexia
Plan of care-
head end elevation
inj levipil 800mg in bd
inj optineuron 1amp
inj monocef 2 lgm iv
inj Vancomycin 500mg in 200ml NS
Inj Neomol 1gm iv sos
inj lorazepam 2cc i.v SOS
tab pcm 650mg
double strength Ors
monitoring vitals 4th bourly
Monitor vitals-4rth hourly
I/O charting
Lumbar puncture was performed and CSF analysis was done to rule out TB MENINGITIS and arachnoiditis



45yrs/male
SOAP NOTES DAY 7
Subjective
No fever spikes
Objective
On examination :
Pt is c/c
Oriented to t/p/p
No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy
Vitalss
PR: 78 bpm, regular
RR: 15cpm
BP: 100/70 mmHg
GRBS: 116 mg/dl
Systemic examination :
CVS:S1,S2 heard
Apex beat:5th ICS
Resp:
BAE+(vesicular breath sounds)
Nvbs heard
Position of trachea- central
P/A: soft, tenderness absent, bowel sounds heard
Cns: No focal deficit
HMF+
SPEECH-NORMAL
MEMORY-intact
No meningeal signs
Pupils-NS RL
MOTOR
Power-(4/5 4/5)
Tone-
Reflexes-
B T S K A P
R 2+ 2 +1 +2 - withdrawal
L 2 +2 +1 +2 - withdrawal
Assessment-
Euvolemic hyposmolar Hyponatremia
SIADH with hyponatremic seizures
Plan of care-
head end elevation
inj levipil 800mg in bd
inj monocef 1gm bd
inj Vancomycin 500mg in 200ml NS
Inj Neomol 1gm iv sos
inj lorazepam 2cc i.v SOS
tab pcm 650mg
double strength Ors
monitoring vitals 4th hourly


{kind=link}
Comments
Post a Comment