case 13 : A 65 year old male, chronic alcoholic with altered sensorium
thanks jancy
A 65 year old male, chronic alcoholic with altered sensorium
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 65 YEAR OLD MALE WITH ALTERED SENSORIUM UNDER EVALUATION
Chief complaints:
• Fever since 2-3 days, associated with generalized weakness.
• Irrelevant talk and drowsiness since 1 day
History of present illness:
. Patient was apparently asymptomatic, 3 days back.
• From the past 3 days, he developed fever, associated with generalized weakness
• Also has history of irrelevant talk and drowsiness since 1 day
• Has history of binge drinking , since 4-5 days, without eating.
• Has no history of headache, cough, vomiting
History of past illness:
• Has history of rt. femur fracture due to fall from a bike 6 months back.
• Similar complaints in the past due to excessive drinking
Treatment history:
• Has undergone a surgery for right femur
• Has no treatment history of DM, HTN, CAD, asthma, stroke, blood transfusion, TB, hormones, antibiotics, chemoradiation.
Personal history:
• Pt is married and is farmer by occupation.
• His appetite is normal, and follows a mixed diet.
• Has regular bowel habits and normal micturition
• Has no known allergies
• He's an alcoholic, consumes alcohol regularly, since 40 years
• Has a habit of smoking chutta since 40 yrs, 4-5 per day
Family history:
• Has no family history of DM, HTN, TB, asthma, cancers, stroke, heart diseases
Physical Examination:
• Has no pallor, no cyanosis, no lymphadenopathy, no clubbing , no oedema of feet, no malnutrition and no dehydration
• Icterus - present

Systemic Examination:
A. Cardiovascular system
• No thrills and no cardiac murmurs
B. Respiratory system
• No dyspnoea and wheeze
. Normal vesicular breath sounds heard
. Position of trachea - central

C. Abdomen
• Shape of abdomen - obese
• Tenderness - present in right hypochondriac and epigastric regions
• Has no palpable mass, bruits, free fluids
• Liver and spleen are not palpable
• Bowel sounds - heard
• Hernial orifices - normal

D. Central Nervous system
• NAD
Investigations :
On 10.8.21
1. ECG

2. Ultrasound report






On 11.8.21
LDH - 1,175.8 IU/L
HCV - positive
Provisional diagnosis:
ALTERED SENSORIUM UNDER EVALUATION
SECONDARY TO ALCOHOLIC INTOXICATION, UTI, PNEUMONIA
? ACUTE VIRAL HEPATITIS( HCV)
Treatment :
On 10.8.21
• IVF 10 NS with 2 ampules thiamine/IV
• INJ. PAN 40 mg/IV / BD
• INJ. Optineuron 1 ampule in 10 NS/IV/OD
• Head end elevation
• Inj. Neomol 1gm/IV infusion
• T. PCM 650 mg
• Monitor BP, PR , RR
• Strict I/O charting
• Tepid sponging and temperature charting 4th hourly
• O2 inhalation @ 15L/min to maintain SPO2 >95%
• IVF - 0.9% NS - Continuous infusion @ 75ml/hr
• Nebulization with BUDECORT /6th hourly
• Syp. LACTULOSE 10ml/BD
> On 11.8.2021 , at 1:30 pm, patient started having tachypnoea with respiratory rate of 44 cpm, and hypoxia ( type 1 respiratory failure)
> Patient suddenly developed weakness of right upper limb and right lower limb with blood pressure of 110/80 mmHg and worsening GCS : E1 V1 M1
> On suspicion of CVA : IC bleed / acute infarct - CT brain was done which showed no significant abnormalities
> Patient was intubated in v/o poor GCS and falling saturations.
But pt had bradycardia and was in asystole for which CPR was initiated according to the aha guidelines, 2015 yet pt couldn't be revived. ECG showed no electrical activity and pt was declared dead at 7:36 pm on 11/8/2021
DEATH SUMMARY
Date of death :11/08/2021
Ward:ICU
Unit:2
Name of Treating Faculty
DR SAI RAGHU (INTERN)
DR LAKSHMI MANASA (INTERN)
DR ROOPA (INTERN)
DR JANCY (INTERN)
DR RAVALI (INTERN)
DR VAMSI KRISHNA PGY1
DR RASHMITHA PGY2
DR NIKITHA PGY2
DR HAREEN (SR)
DR ARJUN KUMAR (AP)
DR RAKESH BISWAS (HOD)
Diagnosis
TYPE 1 RESPIRATORY FAILURE SECONDARY TO PENUMONIA ? ASPIRATION/INFECTIVE ? ACUTE INFARCT IN BRAIN STEM
ALCOHOLIC DELIRIUM
ACUTE VIRAL HEPATITIS( HCV+ve)
? ALCOHOLIC HEPATITIS
Case History and Clinical Findings
A 65 YEAR OLD MALE CHRONIC ALCOHOLIC WITH C/O FEVER SINCE 2-3 DAYS ASSOCIATED WITH GENERALISED WEAKNESS ,IRRELEVANT TALK AND DROWSINESS SINCE 1 DAY.
H/O BINGE DRINKING SINCE 4-5 DAYS WITHOUT EATING
IRRELEVANT TALK AND DROWSINESS SINCE 1 DAY
NO H/O HEADACHE/VOMITING/SEIZURES
NO OTHER COMPLAINTS
NOT A K/C/O OF DIABETES,HYPERTENSION,TB,ASTHMA
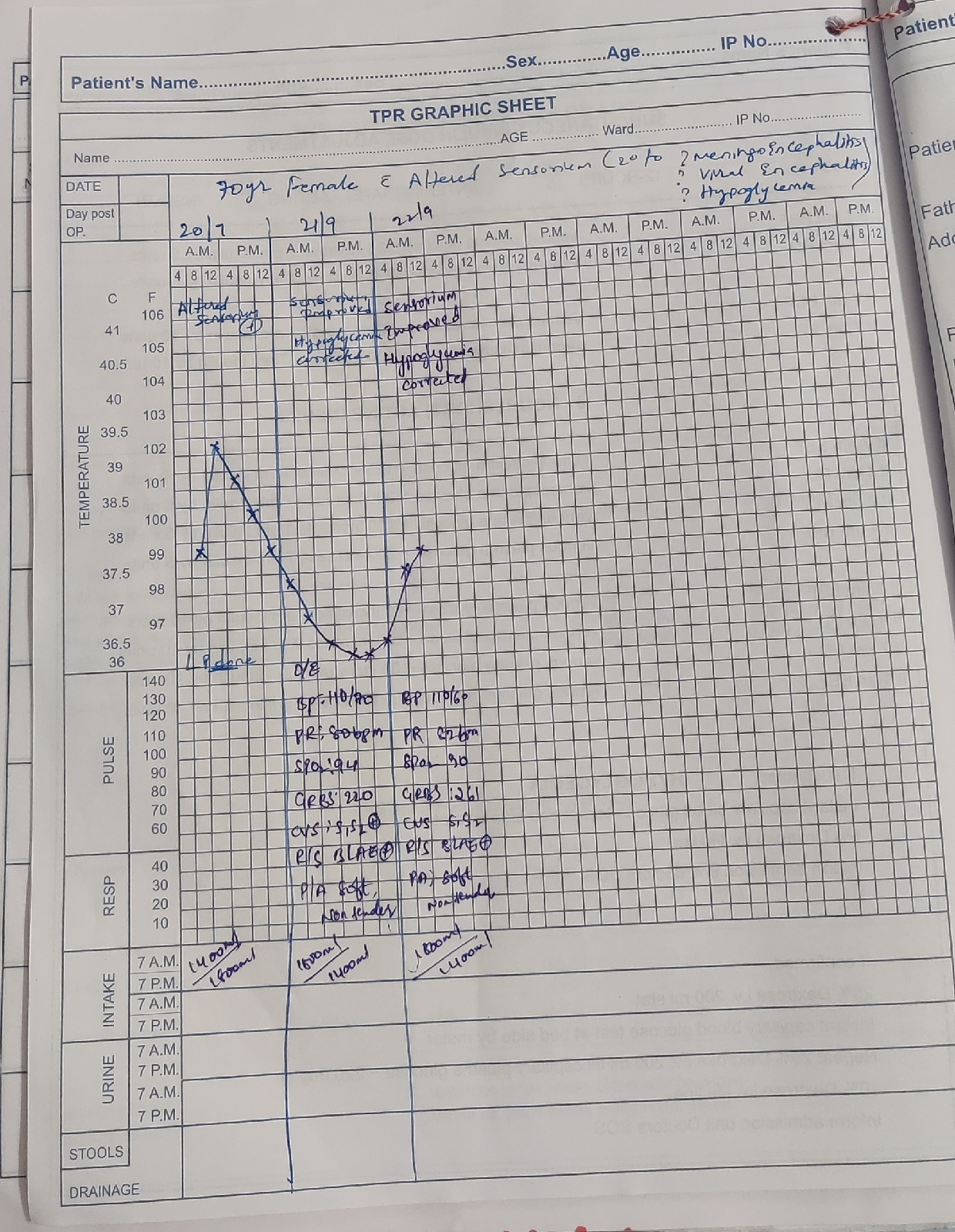
GENERAL EXAMINATION:PATIENT IS CONSCIOUS, NON COOPERATIVE AND NOT WELL ORIENTED TO TIME AND PLACE
TEMP: 100F
PULSE RATE; 141BPM
BP :110/70mmhg
RR- 20cpm
ICTERUS +
NOPALLOR,CYANOSIS,CLUBBING,OEDEMA,GENERALISED LYMPHADENOPATHY
SYSTEMIC EXAMINATION :
CVS: S1S2 HEARD
NO THRILLS AND MURMURS
RESPIRATORY SYSTEM: NVBS +BAE +
PER ABDOMEN :ABDOMEN IS SOFT ,TENDERNESS PRESENT IN RIGHT HYPOCHONDRIUM AND EPIGASTRIC REGION
THERE IS NO PALPABLE MASS
BOWEL SOUNDS +
CENTRAL NERVOUS SYSTEM: GCS: E3 V2 M4.
ALL SUPERFICIAL AND DEEP REFLEXES ARE NORMAL
Treatment Given(Enter only Generic Name)
1.IV FLUIDS
2.INJ.CEFTRIAXONE 1gm IV/BD
3.INJ.PAN 40MG
4.INJ.OPTINEURON 1amp IN 100ml IV/OD
5.IV FLUIDS 0.9%NS CONTINUOUS AT 75ML/HR 6.TAB.PCM 650 MG TID
7.SYP.LACTULOSE 15ML BD
8.INJ. NEOMOL 1GM IV SOS
9.BP/PR/TEMP/SPO2 MONITORING
10.NEB WITH IPRAVENT AND BUDECORT - 6TH HOURLY
11.HEAD END ELEVATION WITH O2 INHALATION AT 3-4 Lit
12.TAB.OLANZEPINE 5MG/H/S
13.T.DOXYCYCLINE 100MG/OD
PATIENT SUDDENLY BECAME UNRESPONSIVE WITH GCS OF E1V1M1( 3/15) HYPOXIC AND TACHYPNEA.
IN V/O POOR GCS AND FALLING SATURTAIONS PATIENT WAS INTUBATED WITH ET 7.0 AND IMMEDIATELY AFTER INTUBATION PATIENT HAD CARDIAC ARREST
BP,PR-NR
CPR WAS INTIATED ACC. TO 2015 AHA GUIDELINES
7:05 PM : BP, PR-NR CPR INITIATED INJ. ADRENALINE 1CC IV/STAT
7:10 PM : BP , PR - NR CPR CONTINUED INJ.ADRENALINE 1CC IV/STAT
7:15 PM : BP , PR - NR CPR CONTINUED INJ.ADRENALINE 1CC IV/STAT
7:20 PM : BP , PR - NR CPR CONTINUED INJ.ADRENALINE 1CC IV/STAT
7:25 PM : BP , PR - NR CPR CONTINUED INJ.ADRENALINE 1CC IV/STAT
7:30 PM : BP , PR - NR CPR CONTINUED INJ.ADRENALINE 1CC IV/STAT
7:35 PM : BP , PR - NR CPR CONTINUED INJ.ADRENALINE 1CC IV/STAT
DESPITE OF THE ABOVE RESUSCITATION MEASURES PATIENT COULD'NT BE REVIVED AND DECLARED DEAD AT 7:36PM ON 11/8/21.
DEATH SUMMARY
A 65 YR OLD MALE PRESENTED TO CASUALTY WITH ALTERED STATE AND GCS E3V2M4 AND PUPILS NSRL
PATIENT ATTENDERS GAVE A HISTORY OF INCREASED INTAKE OF ALCOHOL 6 DAYS WITHOUT FOOD INTAKE
INTEGRATING THE HISTORY AND CLINICAL PRESENTATION A WORKING DIAGNOSIS OF DELIRIUM SECONDARY TO ALCOHOL INTOXICATION WERNICKES ENCEPHALOPATHY ( METABOLIC ETIOLOGY) WAS MADE AND PATIENT WAS GIVEN SUPPORTIVE TREATMENT VITALS BEING STABLE
ON 11/08/2021 AT 1:30 PM ,PATIENT STARTED HAVING TACHYPNEA WITH RESPIRATORY RATE OF 44cpm,(TYPE 1 RESPIRATORY FAILURE )
PATIENT SUDDENLY DEVELOPED WEAKNESS OF RIGHT UPPER LIMB AND LOWER LIMB WITH BLOOD PRESSURE OF 110/80MMHG AND WORSENING GCS E1V1M1.
ON SUSPICION OF CVA IC BLEED/ ACUTE INFARCT
,CT WAS DONE WHICH TURNED OUT TO BE NORMAL AND IN VIEW OF FALLING SATURATIONS, POOR GCS ,PATIENT WAS INTUBATED BUT HE HAD BRADYCARDIA AND WAS ASYSTOLIC FOR WHICH CPR WAS INITIATED ACCORDING TO AHA GUIDELINES 2015,YET PATIENT COULD'NT BE REVIVED AND ECG SHOWED NO
ELECTRICAL ACTIVITY AND PATIENT WAS DECLARED DEAD AT 7:36PM ON 11/8/2021
IMMEDIATE CAUSE OF DEATH :
TYPE 1 RESPIRATORY FAILURE
SECONDARY TO PNEUMONIA
ANTECEDENT CAUSE OF DEATH :
? ACUTE INFARCT INVOLVING BRAIN STEM
ALCOHOLIC DELIRIUM
ACUTE VIRAL HEPATITIS HEP C
ALCOHOLIC HEPATITIS

{kind=link}
Comments
Post a Comment